Liver Transplant Information
Living Donor Liver Transplantation (LDLT)
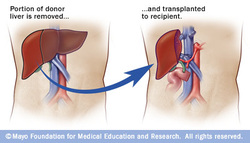
Living donor liver transplantation has emerged in recent decades as a critical surgical option for patients with end stage liver disease. The concept of LDLT is based on (1) the remarkable regenerative capacities of the human liver and (2) the widespread shortage of deceased donor livers for patients awaiting transplant. In LDLT, a piece of healthy liver is surgically removed from a living person and transplanted into a recipient, immediately after the recipient’s diseased liver has been entirely removed.
Historically, LDLT began as a means for parents of children with severe liver disease to donate a portion of their healthy liver to replace their child's entire damaged liver. The first report of successful LDLT was at the University of Chicago Medical Center in November 1989. Surgeons eventually realized that adult-to-adult LDLT was also possible, and now the practice is common in a few reputable medical institutes.
LDLT is considered even more technically demanding than standard deceased donor liver transplantation, which is already one of the most demanding surgeries performed today. It also poses the ethical problems underlying the indication of a major surgical operation on a healthy human being.
In various case series, the risk of complications in the donor is around 10% and very occasionally a second operation is needed. Common problems are biliary fistula, gastric stasis and infections; they are more common after removal of the right lobe of the liver. Death after LDLT has been reported at 0% (Japan), 3% (USA) and <1% (Europe), with risks likely to decrease further as surgeons gain more experience in this procedure.
In a typical adult recipient LDLT, 55 to 70% of the liver (the right lobe) is removed from a healthy living donor. The donor's liver will regenerate approaching 100% function within 4–6 weeks, and will almost reach full volumetric size with recapitulation of the normal structure soon thereafter. It may be possible to remove up to 70% of the liver from a healthy living donor without harm in most cases. The transplanted portion will reach full function and the appropriate size in the recipient as well, although it will take longer than for the donor.
Living donors are faced with risks and/or complications after the surgery. Blood clots and biliary problems have the possibility of arising in the donor post-op, but these issues are remedied fairly easily. Although death is a risk that a living donor must be willing to accept prior to the surgery, the mortality rate of living donors in the United States is low. The LDLT donor's immune system does diminish as a result of the liver regenerating, so certain foods which would normally cause an upset stomach could cause serious illness.
Liver Donor Requirements
Any member of the family, parent, sibling, child, spouse or a volunteer can donate their liver. The criteria for a liver donation include:
Before one becomes a living donor, the donor must undergo testing to ensure that the individual is physically and mentally fit. Sometimes CT scans or MRIs are done to image the liver. In most cases, the work up is done in 2–3 weeks.
Complications
Living donor surgery is done at a major center. Very few individuals require any blood transfusions during or after surgery. Even though the procedure is very safe, all potential donors should know there is a 5 to 10 percent chance of death. Other risks of donating a liver include bleeding, infection, painful incision, possibility of blood clots and a prolonged recovery The vast majority of donors enjoy complete and full recovery within 2–3 months.
Pediatric Transplantation
In children, living liver donor transplantations have become very accepted. The accessibility of adult parents who want to donate a piece of the liver for their children/infants has reduced the number of children who would have otherwise died waiting for a transplant. Having a parent as a donor also has made it a lot easier for children—because both patients are in the same hospital and can help boost each other's morale.
Benefits
There are several advantages of living liver donor transplantation over deceased donor transplantation, including:
Screening for Donors
Living donor transplantation is a multidisciplinary approach. All living liver donors undergo medical evaluation. Every hospital that performs transplants has dedicated nurses who provide specific information about the procedure and answer questions that families may have. During the evaluation process, confidentially is assured on the potential donor. Every effort is made to ensure that organ donation is not made by coercion from other family members. The transplant team provides both thorough counseling and support to the donor and family that continues until full recovery is made.
All donors are assessed medically to ensure that they can undergo the surgery. Blood type of the donor and recipient must be compatible but not always identical. Other things assessed prior to surgery include the anatomy of the donor liver. However, even with mild variations in blood vessels and bile duct, surgeons today are able to perform transplantation without problems. The most important criterion for a living liver donor is to be in excellent health.
Historically, LDLT began as a means for parents of children with severe liver disease to donate a portion of their healthy liver to replace their child's entire damaged liver. The first report of successful LDLT was at the University of Chicago Medical Center in November 1989. Surgeons eventually realized that adult-to-adult LDLT was also possible, and now the practice is common in a few reputable medical institutes.
LDLT is considered even more technically demanding than standard deceased donor liver transplantation, which is already one of the most demanding surgeries performed today. It also poses the ethical problems underlying the indication of a major surgical operation on a healthy human being.
In various case series, the risk of complications in the donor is around 10% and very occasionally a second operation is needed. Common problems are biliary fistula, gastric stasis and infections; they are more common after removal of the right lobe of the liver. Death after LDLT has been reported at 0% (Japan), 3% (USA) and <1% (Europe), with risks likely to decrease further as surgeons gain more experience in this procedure.
In a typical adult recipient LDLT, 55 to 70% of the liver (the right lobe) is removed from a healthy living donor. The donor's liver will regenerate approaching 100% function within 4–6 weeks, and will almost reach full volumetric size with recapitulation of the normal structure soon thereafter. It may be possible to remove up to 70% of the liver from a healthy living donor without harm in most cases. The transplanted portion will reach full function and the appropriate size in the recipient as well, although it will take longer than for the donor.
Living donors are faced with risks and/or complications after the surgery. Blood clots and biliary problems have the possibility of arising in the donor post-op, but these issues are remedied fairly easily. Although death is a risk that a living donor must be willing to accept prior to the surgery, the mortality rate of living donors in the United States is low. The LDLT donor's immune system does diminish as a result of the liver regenerating, so certain foods which would normally cause an upset stomach could cause serious illness.
Liver Donor Requirements
Any member of the family, parent, sibling, child, spouse or a volunteer can donate their liver. The criteria for a liver donation include:
- Being in good health
- Having a blood type that matches or is compatible with the recipient's
- Having a charitable desire of donation without financial motivation
- Being between 18 and 60 years old
- Being of similar or bigger size than the recipient
Before one becomes a living donor, the donor must undergo testing to ensure that the individual is physically and mentally fit. Sometimes CT scans or MRIs are done to image the liver. In most cases, the work up is done in 2–3 weeks.
Complications
Living donor surgery is done at a major center. Very few individuals require any blood transfusions during or after surgery. Even though the procedure is very safe, all potential donors should know there is a 5 to 10 percent chance of death. Other risks of donating a liver include bleeding, infection, painful incision, possibility of blood clots and a prolonged recovery The vast majority of donors enjoy complete and full recovery within 2–3 months.
Pediatric Transplantation
In children, living liver donor transplantations have become very accepted. The accessibility of adult parents who want to donate a piece of the liver for their children/infants has reduced the number of children who would have otherwise died waiting for a transplant. Having a parent as a donor also has made it a lot easier for children—because both patients are in the same hospital and can help boost each other's morale.
Benefits
There are several advantages of living liver donor transplantation over deceased donor transplantation, including:
- Transplant can be done on an elective basis because the donor is readily available.
- There are fewer possibilities for complications and death while waiting for a deceased organ donor.
Screening for Donors
Living donor transplantation is a multidisciplinary approach. All living liver donors undergo medical evaluation. Every hospital that performs transplants has dedicated nurses who provide specific information about the procedure and answer questions that families may have. During the evaluation process, confidentially is assured on the potential donor. Every effort is made to ensure that organ donation is not made by coercion from other family members. The transplant team provides both thorough counseling and support to the donor and family that continues until full recovery is made.
All donors are assessed medically to ensure that they can undergo the surgery. Blood type of the donor and recipient must be compatible but not always identical. Other things assessed prior to surgery include the anatomy of the donor liver. However, even with mild variations in blood vessels and bile duct, surgeons today are able to perform transplantation without problems. The most important criterion for a living liver donor is to be in excellent health.
